
Deanna is an ACE® certified personal trainer, Balanced Body® Pilates instructor, and NASM® Fitness Nutrition Specialist. She is passionate about inspiring others to lead a healthier lifestyle through fun workouts and healthy food. When she’s not creating new workouts and recipes for her blog The Live Fit Girls she enjoys running with her two dogs and traveling.

Hip flexors. These hardworking muscles are crucial in foundational movements such as sitting, standing, walking and running — they act as a bridge connecting your torso to your lower body. Some muscles in this group can be notoriously weak or tight and those of you who have ever had issues with this part of your body will know the uncomfortable pain of either all too well. There’s a lot of debate in the world of sports science over how much you should strengthen and stretch your hip flexors — we’ll explain.
Vertebroplasty and kyphoplasty are minimally invasive treatments to repair compression fractures of the vertebrae caused by osteoporosis. Vertebroplasty uses three-dimensional imaging to assist in guiding a fine needle through the skin into the vertebral body, the largest part of the vertebrae. A glue-like bone cement is then injected into the vertebral body space, which quickly hardens to stabilize and strengthen the bone and provide pain relief. In kyphoplasty, prior to injecting the bone cement, a special balloon is inserted and gently inflated to restore height to the vertebral structure and reduce spinal deformity.
Hip tendonitis is inflammation of any of the hip tendons, or thick cords that attach muscles to bone. Similar to strains, hip tendonitis is commonly caused by overuse. And, also like strains, tendonitis frequently affects the same population—athletes who participate in cycling, swimming, running, and other sports that repeatedly stress the hip. High intensity interval training (HIIT) workouts and other activities that involve a high volume of kicking, squatting, and jumping can also lead to tendon inflammation.
Marvelously progressive, concise, and cogent guidelines for physicians on the treatment of low back pain. These guidelines almost entirely “get it right” in my opinion, and are completely consistent with recommendations I’ve been making for years on PainScience.com. They are particularly to be praised for strongly discouraging physicians from ordering imaging tests only “for patients with low back pain when severe or progressive neurologic deficits are present or when serious underlying conditions are suspected.”
The condition is cauda equina syndrome. It involves “acute loss of function of the neurologic elements (nerve roots) of the spinal canal below the termination (conus) of the spinal cord,” where the nerves spread out like a horse (equina) tail. Again, this condition causes symptoms in the “saddle” of the body: butt, groin, inner thighs. BACK TO TEXT
Emerging technologies such as X-rays gave physicians new diagnostic tools, revealing the intervertebral disc as a source for back pain in some cases. In 1938, orthopedic surgeon Joseph S. Barr reported on cases of disc-related sciatica improved or cured with back surgery.[100] As a result of this work, in the 1940s, the vertebral disc model of low back pain took over,[99] dominating the literature through the 1980s, aiding further by the rise of new imaging technologies such as CT and MRI.[100] The discussion subsided as research showed disc problems to be a relatively uncommon cause of the pain. Since then, physicians have come to realize that it is unlikely that a specific cause for low back pain can be identified in many cases and question the need to find one at all as most of the time symptoms resolve within 6 to 12 weeks regardless of treatment.[99]

Key objects. If frequently used objects are too far out of arm’s reach, it can result in repeated twisting that can strain your lower back. To avoid this, keep things you use the most within easy reach. This could include your phone, stapler, pens, notepads, or anything else that gets regular use. If something is too large or heavy to keep near your keyboard, place it where you have to stand to get it to help you resist the urge to twist.
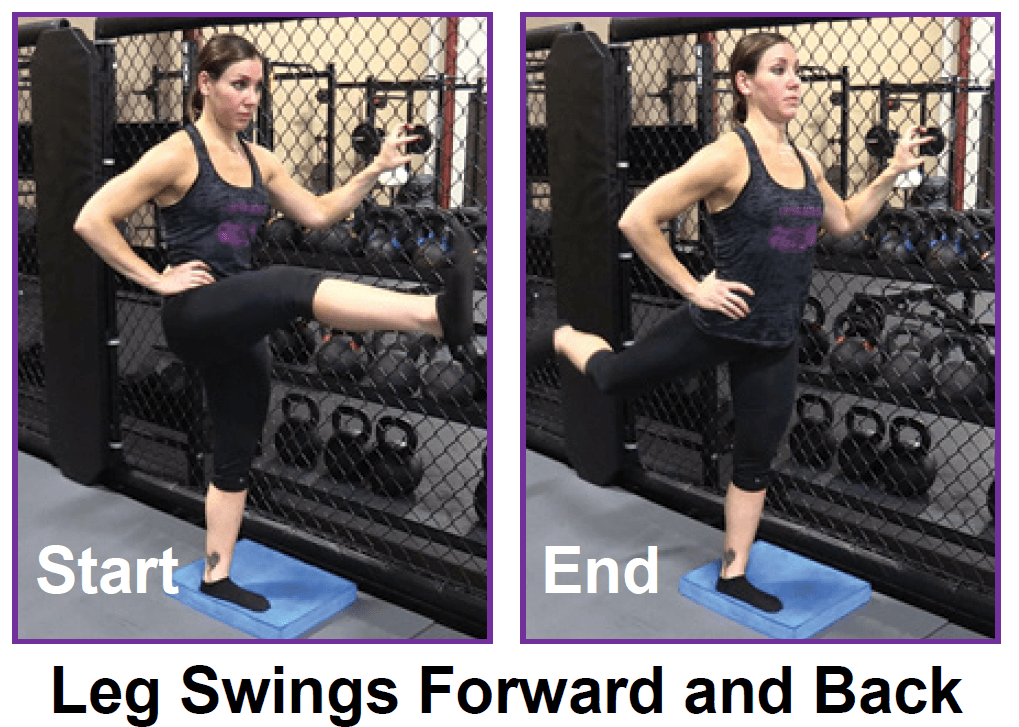
To help you strengthen these important muscles, Miranda put together a list of exercises, below. They include dynamic warm-up moves, meant to activate your hip muscles and prep them for the bigger movements to come; functional moves that train basic movement patterns, like the squat, hip hinge, and lunge; functional plyometric exercises that train explosive power; and a few moves that get you moving in different planes of motion, or directions. 
If you’re someone who’s got a good stretching routine down, both before and after a HIIT workout, bike ride or run, odds are the discomfort you feel indicates that there are grounds for more strengthening exercises. It’s important to add that many yogis with extremely flexible hips run into overstretching injuries like hip flexor strains. But, these injuries aren’t just limited to the uber-flexible. Runners, cyclists, and Stairmaster lovers might strain these muscles due to frequent overuse. We’ll share a hip flexor workout below but, first up, some stretches.
Stop searching for a miracle cure for your back pain. We’ve all seen the advertisements that promise a miracle cure for your low back pain. Hanging by your feet on an inversion table, rubbing healing balms on your back or spending money on fancy computerized traction devices all sound effective but the evidence indicates that many of these miracle cures are not beneficial.
Apply the above concept to your hips. When you sit, your hips are in a "flexed" position. Therefore, the muscles that flex your hips are in a shortened state. You probably spend at least a third of your day sitting down. Think about how much time those hip flexor muscles stay shortened. A lot. Over time, they become tighter and tighter until you look like the old man in the picture. So unless you want to look like that, perform the stretches shown below.
The hip is a common site of osteoarthritis. To help protect the hip joint from "wear and tear," it is important to strengthen the muscles that support it. Your hip also controls the position of your knee, and strengthening your hips may be one component of your rehab program for knee pain. Your physical therapist may also prescribe hip exercises after total hip replacement if you have a hip labrum tear or as part of your hip exercise program for hip pain.
Start kneeling on your mat with knees hip-width apart and hips directly over knees. Press your shins and the tops of your feet into the mat. Bring your hands to your low back, fingers pointing down, and rest palms above glutes. Inhale and lift your chest, and then slowly start to lean your torso back. From here, bring your right hand to rest on your right heel and then your left hand to your left heel. (If you can't reach your heels, turn your toes under; it will be easier to reach your heels in this modification.) Press your thighs forward so they are perpendicular to the floor. Keep your head in a relatively neutral position or, if it doesn't strain your neck, drop it back. Hold for 30 seconds. To come out of the pose, bring your hands to your hips and slowly, leading with your chest, lift your torso as you press the thighs down toward the floor.

