
Iliopsoas syndrome, which is also called psoas syndrome or iliopsoas tendonitis, occurs when the iliopsoas muscles are injured. Lower back pain is the most common symptom; however, pain can also occur in the hip, thigh, or leg. The iliopsoas bursa, which is a fluid-filled sac located on the inside of the hip that reduces rubbing and friction, is also likely to become inflamed due to the proximity of the two structures. When this happens, the inflamed bursae will make it difficult to move.
The hip flexors are the group of muscles that allow you to lift your knees toward your chest and bend forward from the hips. What is collectively referred to as the hip flexors is actually a group of muscles that includes the iliopsoas, the thigh muscles (rectus femoris, Sartorius and tensor fasciae latae), and the inner thigh muscles (adductor longus and brevis, pectineus and gracilis).
Shingles (herpes zoster) is an acute infection of the nerves that supply sensation to the skin, generally at one or several spinal levels and on one side of the body (right or left). Patients with shingles usually have had chickenpox earlier in life. The herpes virus that causes chickenpox is believed to exist in a dormant state within the spinal nerve roots long after the chickenpox resolves. In people with shingles, this virus reactivates to cause infection along the sensory nerve, leading to nerve pain and usually an outbreak of shingles (tiny blisters on the same side of the body and at the same nerve level). The back pain in patients with shingles of the lumbar area can precede the skin rash by days. Successive crops of tiny blisters can appear for several days and clear with crusty inflammation in one to two weeks. Patients occasionally are left with a more chronic nerve pain (postherpetic neuralgia). Treatment can involve symptomatic relief with lotions, such as calamine, or medications, such as acyclovir (Zovirax), for the infection and pregabalin (Lyrica) or lidocaine (Lidoderm) patches for the pain.

To ease the pain and lower your odds of an injury, don’t try to do too much at once. “Start with just 10 minutes,” says Arina Garg, MD, a rheumatology fellow at The Center for Excellence for Arthritis and Rheumatology at the Louisiana University Health Sciences Center. “Every few days, increase that time by 5 to 10 minutes.” Your goal is to work up to 30 minutes of aerobic exercise, 5 days a week.
Shingles (herpes zoster) is an acute infection of the nerves that supply sensation to the skin, generally at one or several spinal levels and on one side of the body (right or left). Patients with shingles usually have had chickenpox earlier in life. The herpes virus that causes chickenpox is believed to exist in a dormant state within the spinal nerve roots long after the chickenpox resolves. In people with shingles, this virus reactivates to cause infection along the sensory nerve, leading to nerve pain and usually an outbreak of shingles (tiny blisters on the same side of the body and at the same nerve level). The back pain in patients with shingles of the lumbar area can precede the skin rash by days. Successive crops of tiny blisters can appear for several days and clear with crusty inflammation in one to two weeks. Patients occasionally are left with a more chronic nerve pain (postherpetic neuralgia). Treatment can involve symptomatic relief with lotions, such as calamine, or medications, such as acyclovir (Zovirax), for the infection and pregabalin (Lyrica) or lidocaine (Lidoderm) patches for the pain.

Start kneeling on your mat with knees hip-width apart and hips directly over knees. Press your shins and the tops of your feet into the mat. Bring your hands to your low back, fingers pointing down, and rest palms above glutes. Inhale and lift your chest, and then slowly start to lean your torso back. From here, bring your right hand to rest on your right heel and then your left hand to your left heel. (If you can't reach your heels, turn your toes under; it will be easier to reach your heels in this modification.) Press your thighs forward so they are perpendicular to the floor. Keep your head in a relatively neutral position or, if it doesn't strain your neck, drop it back. Hold for 30 seconds. To come out of the pose, bring your hands to your hips and slowly, leading with your chest, lift your torso as you press the thighs down toward the floor.
Really a great content. Let me tell you first about hip flexor it is the engine through which our body moves. They control balance, our ability to sit, stand, twist, reach, bend, walk and step. One of my patient also suffering from same problem but due to lack of money he was unable to afford a treatment. So i recommend him a program to unlock hip flexor. If anyone wants they can check it out here ;- https://tinyurl.com/y8yaqs2s Report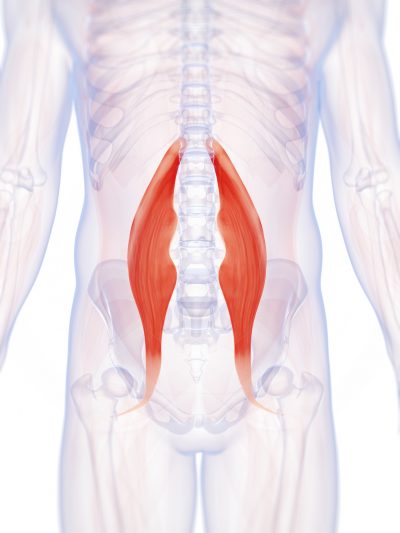
Paget's disease can be diagnosed on plain X-rays. However, a bone biopsy is occasionally necessary to ensure the accuracy of the diagnosis. Bone scanning is helpful to determine the extent of the disease, which can involve more than one bone area. A blood test, alkaline phosphatase, is useful for diagnosis andmonitoring response to therapy. Treatment options include aspirin, other anti-inflammatory medicines, pain medications, and medications that slow therate of bone turnover, such as calcitonin (Calcimar, Miacalcin), etidronate (Didronel), alendronate (Fosamax), risedronate (Actonel), and pamidronate (Aredia).
Eleven updates have been logged for this article since publication (2009). All PainScience.com updates are logged to show a long term commitment to quality, accuracy, and currency. more When’s the last time you read a blog post and found a list of many changes made to that page since publication? Like good footnotes, this sets PainScience.com apart from other health websites and blogs. Although footnotes are more useful, the update logs are important. They are “fine print,” but more meaningful than most of the comments that most Internet pages waste pixels on.

Bony encroachment: Any condition that results in movement or growth of the vertebrae of the lumbar spine can limit the space (encroachment) for the adjacent spinal cord and nerves. Causes of bony encroachment of the spinal nerves include foraminal narrowing (narrowing of the portal through which the spinal nerve passes from the spinal column, out of the spinal canal to the body, commonly as a result of arthritis), spondylolisthesis (slippage of one vertebra relative to another), and spinal stenosis (compression of the nerve roots or spinal cord by bony spurs or other soft tissues in the spinal canal). Spinal-nerve compression in these conditions can lead to sciatica pain that radiates down the lower extremities. Spinal stenosis can cause lower-extremity pains that worsen with walking and are relieved by resting (mimicking the pains of poor circulation). Treatment of these afflictions varies, depending on their severity, and ranges from rest and exercises to epidural cortisone injections and surgical decompression by removing the bone that is compressing the nervous tissue.

If you are experiencing true numbness14 around the groin and buttocks and/or failure of bladder or bowel control, please consider it a serious emergency — do not wait to see if it goes away. These symptoms indicate spinal cord injury or compression15 and require immediate medical attention. (Few people will have symptoms like this without having already decided it’s an emergency, but I have to cover all the bases here.)
The hip is a common site of osteoarthritis. To help protect the hip joint from "wear and tear," it is important to strengthen the muscles that support it. Your hip also controls the position of your knee, and strengthening your hips may be one component of your rehab program for knee pain. Your physical therapist may also prescribe hip exercises after total hip replacement if you have a hip labrum tear or as part of your hip exercise program for hip pain.

Degenerative disc disease. At birth, intervertebral discs are full of water and at their healthiest. As people age over time, discs lose hydration and wear down. As the disc loses hydration, it cannot resist forces as well, and transfers force to the disc wall that may develop tears and cause pain or weakening that can lead to a herniation. The disc can also collapse and contribute to stenosis.
Imaging is indicated when there are red flags, ongoing neurological symptoms that do not resolve, or ongoing or worsening pain.[5] In particular, early use of imaging (either MRI or CT) is recommended for suspected cancer, infection, or cauda equina syndrome.[5] MRI is slightly better than CT for identifying disc disease; the two technologies are equally useful for diagnosing spinal stenosis.[5] Only a few physical diagnostic tests are helpful.[5] The straight leg raise test is almost always positive in those with disc herniation.[5] Lumbar provocative discography may be useful to identify a specific disc causing pain in those with chronic high levels of low back pain.[41] Similarly, therapeutic procedures such as nerve blocks can be used to determine a specific source of pain.[5] Some evidence supports the use of facet joint injections, transforminal epidural injections and sacroilliac injections as diagnostic tests.[5] Most other physical tests, such as evaluating for scoliosis, muscle weakness or wasting, and impaired reflexes, are of little use.[5]
Injury to the bones and joints: Fractures (breakage of bone) of the lumbar spine and sacrum bone most commonly affect elderly people with osteoporosis, especially those who have taken long-term cortisone medication. For these individuals, occasionally even minimal stresses on the spine (such as bending to tie shoes) can lead to bone fracture. In this setting, the vertebra can collapse (vertebral compression fracture). The fracture causes an immediate onset of severe localized pain that can radiate around the waist in a band-like fashion and is made intensely worse with body motions. This pain generally does not radiate down the lower extremities. Vertebral fractures in younger patients occur only after severe trauma, such as from motor-vehicle accidents or a convulsive seizure.
In terms of diagnosing hip pain, typically a patient will expect when they come in to be asked about their symptoms, and it’s very important to find out when did these symptoms start, how long they have been going on, how frequent they are, if they come on in the morning or the evening, do they come on with any certain activity, and if there is something that makes it better or worse. The intensity of the pain is also important. Does it have any associated radiating symptoms? Is it localized in one spot or does it move? After getting a history and finding out what type of pain the patient is having, which also includes whether the pain is dull, aching, sharp, or intense, then it’s important to do a good physical exam. The physical examination involves testing the muscle strength, testing for sensation, doing provocative maneuvers which might help us rule out one type of injury from another.
The treatment of lumbar strain consists of resting the back (to avoid reinjury), medications to relieve pain and muscle spasm, local heat applications, massage, and eventual (after the acute episode resolves) reconditioning exercises to strengthen the low back and abdominal muscles. Initial treatment at home might include heat application, acetaminophen (Tylenol) or ibuprofen (Advil, Motrin), and avoiding reinjury and heavy lifting. Prescription medications that are sometimes used for acute low back pain include anti-inflammatory medications, such as sulindac (Clinoril), naproxen (Naprosyn), and ketorolac (Toradol) by injection or by mouth, muscle relaxants, such as carisoprodol (Soma), cyclobenzaprine (Flexeril), methocarbamol (Robaxin), and metaxalone (Skelaxin), as well as analgesics, such as tramadol (Ultram).
Shingles (herpes zoster) is an acute infection of the nerves that supply sensation to the skin, generally at one or several spinal levels and on one side of the body (right or left). Patients with shingles usually have had chickenpox earlier in life. The herpes virus that causes chickenpox is believed to exist in a dormant state within the spinal nerve roots long after the chickenpox resolves. In people with shingles, this virus reactivates to cause infection along the sensory nerve, leading to nerve pain and usually an outbreak of shingles (tiny blisters on the same side of the body and at the same nerve level). The back pain in patients with shingles of the lumbar area can precede the skin rash by days. Successive crops of tiny blisters can appear for several days and clear with crusty inflammation in one to two weeks. Patients occasionally are left with a more chronic nerve pain (postherpetic neuralgia). Treatment can involve symptomatic relief with lotions, such as calamine, or medications, such as acyclovir (Zovirax), for the infection and pregabalin (Lyrica) or lidocaine (Lidoderm) patches for the pain.
Start kneeling on your mat with knees hip-width apart and hips directly over knees. Press your shins and the tops of your feet into the mat. Bring your hands to your low back, fingers pointing down, and rest palms above glutes. Inhale and lift your chest, and then slowly start to lean your torso back. From here, bring your right hand to rest on your right heel and then your left hand to your left heel. (If you can't reach your heels, turn your toes under; it will be easier to reach your heels in this modification.) Press your thighs forward so they are perpendicular to the floor. Keep your head in a relatively neutral position or, if it doesn't strain your neck, drop it back. Hold for 30 seconds. To come out of the pose, bring your hands to your hips and slowly, leading with your chest, lift your torso as you press the thighs down toward the floor.

Osteoarthritis. This condition results from wear and tear of the disc and facet joints. It causes pain, inflammation, instability, and stenosis to a variable degree, and can occur at a single level or multiple levels of the lower spine. Spinal osteoarthritis is associated with aging and is slowly progressive. It is also referred to as spondylosis or degenerative joint disease.
Marvelously progressive, concise, and cogent guidelines for physicians on the treatment of low back pain. These guidelines almost entirely “get it right” in my opinion, and are completely consistent with recommendations I’ve been making for years on PainScience.com. They are particularly to be praised for strongly discouraging physicians from ordering imaging tests only “for patients with low back pain when severe or progressive neurologic deficits are present or when serious underlying conditions are suspected.”
For the 31 million Americans who suffer from daily back pain, relief can be hard to find. In fact, back pain is the single leading cause of disability worldwide and the second most common reason for visits to the doctor. While it can be caused by many different things—extended periods of sitting or standing at work, bad posture, stress, an overly-strenuous workout or helping a friend move, to mention a few—once back pain hits, it can stick around for a long time. Your gut instinct might be to stay frozen until it goes away, but the best thing for your back is to keep it moving with gentle stretches. In fact, a regular routine of a few quick exercises can help you reduce your back pain without a trip to the doctor. Try to do the following exercises every morning and again at night.
Stand tall with your hips square and bend your right knee, bringing your foot towards your bum. Grab the right foot with your right hand and actively pull the foot closer to your glutes. As you do this, send the right knee down towards the ground and keep both knees together. squeeze your butt to promote a posterior pelvic tilt and hold — then switch sides.
