Bony encroachment: Any condition that results in movement or growth of the vertebrae of the lumbar spine can limit the space (encroachment) for the adjacent spinal cord and nerves. Causes of bony encroachment of the spinal nerves include foraminal narrowing (narrowing of the portal through which the spinal nerve passes from the spinal column, out of the spinal canal to the body, commonly as a result of arthritis), spondylolisthesis (slippage of one vertebra relative to another), and spinal stenosis (compression of the nerve roots or spinal cord by bony spurs or other soft tissues in the spinal canal). Spinal-nerve compression in these conditions can lead to sciatica pain that radiates down the lower extremities. Spinal stenosis can cause lower-extremity pains that worsen with walking and are relieved by resting (mimicking the pains of poor circulation). Treatment of these afflictions varies, depending on their severity, and ranges from rest and exercises to epidural cortisone injections and surgical decompression by removing the bone that is compressing the nervous tissue.

To ease the pain and lower your odds of an injury, don’t try to do too much at once. “Start with just 10 minutes,” says Arina Garg, MD, a rheumatology fellow at The Center for Excellence for Arthritis and Rheumatology at the Louisiana University Health Sciences Center. “Every few days, increase that time by 5 to 10 minutes.” Your goal is to work up to 30 minutes of aerobic exercise, 5 days a week.
How to: Sit down with your knees bent and feet flat on the floor in front of you (a). Place your right ankle on top of your left thigh and flex your right foot (b). Put your hands behind your body, fingertips facing away from your body and begin to press your hips toward your heels until you feel a stretch through your outer left hip. Keep your back tall and chest open (c). Hold for six to eight breaths, then repeat on the other side.
Bony encroachment: Any condition that results in movement or growth of the vertebrae of the lumbar spine can limit the space (encroachment) for the adjacent spinal cord and nerves. Causes of bony encroachment of the spinal nerves include foraminal narrowing (narrowing of the portal through which the spinal nerve passes from the spinal column, out of the spinal canal to the body, commonly as a result of arthritis), spondylolisthesis (slippage of one vertebra relative to another), and spinal stenosis (compression of the nerve roots or spinal cord by bony spurs or other soft tissues in the spinal canal). Spinal-nerve compression in these conditions can lead to sciatica pain that radiates down the lower extremities. Spinal stenosis can cause lower-extremity pains that worsen with walking and are relieved by resting (mimicking the pains of poor circulation). Treatment of these afflictions varies, depending on their severity, and ranges from rest and exercises to epidural cortisone injections and surgical decompression by removing the bone that is compressing the nervous tissue.
Shingles (herpes zoster) is an acute infection of the nerves that supply sensation to the skin, generally at one or several spinal levels and on one side of the body (right or left). Patients with shingles usually have had chickenpox earlier in life. The herpes virus that causes chickenpox is believed to exist in a dormant state within the spinal nerve roots long after the chickenpox resolves. In people with shingles, this virus reactivates to cause infection along the sensory nerve, leading to nerve pain and usually an outbreak of shingles (tiny blisters on the same side of the body and at the same nerve level). The back pain in patients with shingles of the lumbar area can precede the skin rash by days. Successive crops of tiny blisters can appear for several days and clear with crusty inflammation in one to two weeks. Patients occasionally are left with a more chronic nerve pain (postherpetic neuralgia). Treatment can involve symptomatic relief with lotions, such as calamine, or medications, such as acyclovir (Zovirax), for the infection and pregabalin (Lyrica) or lidocaine (Lidoderm) patches for the pain.
Exercise appears to be useful for preventing low back pain.[47] Exercise is also probably effective in preventing recurrences in those with pain that has lasted more than six weeks.[1][48] Medium-firm mattresses are more beneficial for chronic pain than firm mattresses.[49] There is little to no evidence that back belts are any more helpful in preventing low back pain than education about proper lifting techniques.[47][50] Shoe insoles do not help prevent low back pain.[47][51]
Sciatica is a form of radiculopathy caused by compression of the sciatic nerve, the large nerve that travels through the buttocks and extends down the back of the leg. This compression causes shock-like or burning low back pain combined with pain through the buttocks and down one leg, occasionally reaching the foot. In the most extreme cases, when the nerve is pinched between the disc and the adjacent bone, the symptoms may involve not only pain, but numbness and muscle weakness in the leg because of interrupted nerve signaling. The condition may also be caused by a tumor or cyst that presses on the sciatic nerve or its roots.

Sciatica is a form of radiculopathy caused by compression of the sciatic nerve, the large nerve that travels through the buttocks and extends down the back of the leg. This compression causes shock-like or burning low back pain combined with pain through the buttocks and down one leg, occasionally reaching the foot. In the most extreme cases, when the nerve is pinched between the disc and the adjacent bone, the symptoms may involve not only pain, but numbness and muscle weakness in the leg because of interrupted nerve signaling. The condition may also be caused by a tumor or cyst that presses on the sciatic nerve or its roots.
Start kneeling on your mat with knees hip-width apart and hips directly over knees. Press your shins and the tops of your feet into the mat. Bring your hands to your low back, fingers pointing down, and rest palms above glutes. Inhale and lift your chest, and then slowly start to lean your torso back. From here, bring your right hand to rest on your right heel and then your left hand to your left heel. (If you can't reach your heels, turn your toes under; it will be easier to reach your heels in this modification.) Press your thighs forward so they are perpendicular to the floor. Keep your head in a relatively neutral position or, if it doesn't strain your neck, drop it back. Hold for 30 seconds. To come out of the pose, bring your hands to your hips and slowly, leading with your chest, lift your torso as you press the thighs down toward the floor.

Sit in a chair with good lumbar support and proper position and height for the task. Keep shoulders back. Switch sitting positions often and periodically walk around the office or gently stretch muscles to relieve tension. A pillow or rolled-up towel placed behind the small of the back can provide some lumbar support. During prolonged periods of sitting, elevate feet on a low stool or a stack of books.

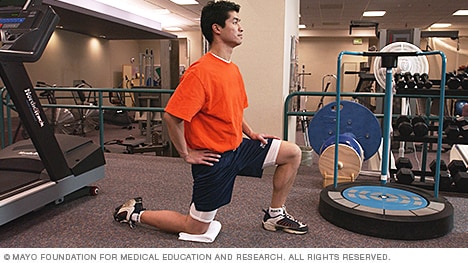
If you’re someone who’s got a good stretching routine down, both before and after a HIIT workout, bike ride or run, odds are the discomfort you feel indicates that there are grounds for more strengthening exercises. It’s important to add that many yogis with extremely flexible hips run into overstretching injuries like hip flexor strains. But, these injuries aren’t just limited to the uber-flexible. Runners, cyclists, and Stairmaster lovers might strain these muscles due to frequent overuse. We’ll share a hip flexor workout below but, first up, some stretches.
To ease the pain and lower your odds of an injury, don’t try to do too much at once. “Start with just 10 minutes,” says Arina Garg, MD, a rheumatology fellow at The Center for Excellence for Arthritis and Rheumatology at the Louisiana University Health Sciences Center. “Every few days, increase that time by 5 to 10 minutes.” Your goal is to work up to 30 minutes of aerobic exercise, 5 days a week.
Lie on your back with your knees bent and your feet flat on the floor. Tighten the muscles in your buttocks, then lift your hips off the ground and hold for about five seconds before slowly lowering yourself back down. Be sure to breathe throughout the exercise. As with the first exercise, you can work up to doing 30 repetitions, resting for a few seconds (or longer) between each. “If you start to get tired, stop and rest for a couple of minutes,” Pariser says.

NINDS-funded studies are contributing to a better understanding of why some people with acute low back pain recover fully while others go on to develop chronic low back pain. Brain imaging studies suggest that people with chronic low back pain have changes in brain structure and function. In one study, people with subacute back pain were followed for one year. Researchers found that certain patterns of functional connectivity across brain networks correlated with the likelihood of pain becoming chronic. The findings suggest that such patterns may help predict who is most likely to transition from subacute to chronic back pain. Other research seeks to determine the role of brain circuits important for emotional and motivational learning and memory in this transition, in order to identify new preventive interventions.
Workers who experience acute low back pain as a result of a work injury may be asked by their employers to have x-rays.[102] As in other cases, testing is not indicated unless red flags are present.[102] An employer's concern about legal liability is not a medical indication and should not be used to justify medical testing when it is not indicated.[102] There should be no legal reason for encouraging people to have tests which a health care provider determines are not indicated.[102]
Don’t medically investigate back pain until it’s met at least three criteria: (1) it’s been bothering you for more than about 6 weeks; (2) it’s severe and/or not improving, or actually getting worse; and (3) there’s at least one other “red flag” (age over 55 or under 20, painful to light tapping, fever/malaise, weight loss, slow urination, incontinence, groin numbness, a dragging toe, or symptoms in both legs like numbness and/or tingling and/or weakness).
The National Institute of Neurological Disorders and Stroke (NINDS) is a component of the National Institutes of Health (NIH) and is the leading federal funder of research on disorders of the brain and nervous system. As a primary supporter of research on pain and pain mechanisms, NINDS is a member of the NIH Pain Consortium, which was established to promote collaboration among the many NIH Institutes and Centers with research programs and activities addressing pain. On an even broader scale, NIH participates in the Interagency Pain Research Coordinating Committee, a federal advisory committee that coordinates research across other U.S. Department of Health and Human Services agencies as well as the Departments of Defense and Veterans Affairs.
Low back pain has been with humans since at least the Bronze Age. The oldest known surgical treatise – the Edwin Smith Papyrus, dating to about 1500 BCE – describes a diagnostic test and treatment for a vertebral sprain. Hippocrates (c. 460 BCE – c. 370 BCE) was the first to use a term for sciatic pain and low back pain; Galen (active mid to late second century CE) described the concept in some detail. Physicians through the end of the first millennium did not attempt back surgery and recommended watchful waiting. Through the Medieval period, folk medicine practitioners provided treatments for back pain based on the belief that it was caused by spirits.[99]
The lumbar (or lower back) region is made up of five vertebrae (L1–L5), sometimes including the sacrum. In between these vertebrae are fibrocartilaginous discs, which act as cushions, preventing the vertebrae from rubbing together while at the same time protecting the spinal cord. Nerves come from and go to the spinal cord through specific openings between the vertebrae, providing the skin with sensations and messages to muscles. Stability of the spine is provided by the ligaments and muscles of the back and abdomen. Small joints called facet joints limit and direct the motion of the spine.[30]
When I do a deep knee bend like a sumo squat I get a popping in the outside of my left knee. It feels like a big tendon or ligament is slipping per something. It isn’t painful peer se but I’m afraid if I do it a lot it will be. Is that a relatively common symptom for a guy with tight flexors, it bands, etc? Should I just push through it or have it checked out?

You'll need a resistance band for this one. With this exercise you're focusing on four movements—flexion, extension, abduction and adduction. Try and stand up straight while doing the exercise. If you have to lean excessively, step closer to the anchor point of your band to decrease resistance. You'll find that not only are you working the muscles of the leg that's moving, the muscles of your stance leg will work quite hard stabilizing and balancing.
Doing the bridge exercise in the morning gets your muscles working, activated, and engaged and will help support you the rest of the day, says Humphrey. Lie on your back with your legs bent and your feet flat on the floor, hip-width apart. Press down through your ankles and raise your buttocks off the floor while you tighten your abdominal muscles. Keep your knees aligned with your ankles and aim for a straight line from knees to shoulders, being sure not to arch your back; hold this position for three to five seconds and then slowly lower your buttocks back to the floor. Start with one set of 10 and build up to two or three sets.
Start in a runner’s lunge with right leg forward, right knee over right ankle and back leg straight. Walk right foot over toward left hand, then drop right shin and thigh to the floor, making sure to keep right knee in line with right hip. Allow left leg to rest on the floor with top of left foot facing down. Take a moment to square your hips to the front of the room. Hold here, or hinge at hips and lower torso toward floor, allowing head to rest on forearms. Hold for at least 30 seconds, then repeat on opposite side. You want to feel a moderate stretch in the outside of the right thigh, but if this pose hurts your knees or feels too uncomfortable, stick with Thread the Needle.

Or anything else. Pain is a poor indicator, period! The human nervous system is really terrible about this: it routinely produces false alarms, and alarms that are much too loud. See Pain is Weird: Pain science reveals a volatile, misleading sensation that is often more than just a symptom, and sometimes worse than whatever started it. BACK TO TEXT

^ Jump up to: a b c d e f Qaseem, A; Wilt, TJ; McLean, RM; Forciea, MA; Clinical Guidelines Committee of the American College of, Physicians. (4 April 2017). "Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians". Annals of Internal Medicine. 166 (7): 514–530. doi:10.7326/M16-2367. PMID 28192789.