
5. Feel free as a bird. Open up those hips with yoga’s pigeon pose! Start on all fours with hands below the shoulders and knees below the hips. Bring the right knee forward until it touches the right hand and place the leg flat on the ground across the body (the right foot is now on the left side of the body, parallel to the front of the mat). Drop left leg to the ground, and extend it back with toes turned under. Keep the hips level, inhale, and walk hands forward. Exhale, and fold the torso over, lowering elbows to the floor. Stay in this position for 5-10 breaths before coming back up to switch sides.
Low and lower back pain can vary from dull pain that develops gradually to sudden, sharp or persistent pain felt below the waist. Unfortunately, almost everyone, at some point during life will experience low back pain that may travel downward into the buttocks and sometimes into one or both lower extremities. The most common cause is muscle strain often related to heavy physical labor, lifting or forceful movement, bending or twisting into awkward positions, or standing in one position too long.
Some of these red flags are much less red than others, especially depending on the circumstances. For instance, “weight loss” is common and often the sign of successful diet! (Well, at least temporarily successful, anyway. 😃) Obviously, if you know of a harmless reason why you have a red flag symptom, it isn’t really a red flag (duh!). But every single actual red flag — in combination with severe low back pain that’s been going on for several weeks — is definitely a good reason to get yourself checked out.
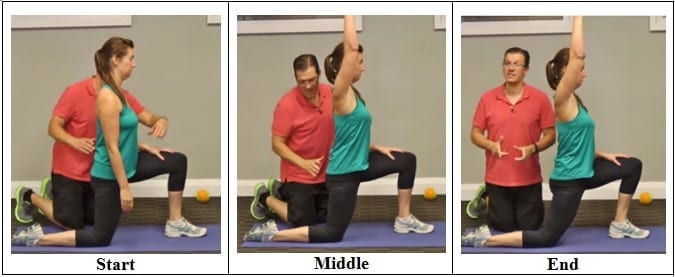
Start in a runner’s lunge, right leg forward with knee over ankle and left knee on ground with top of your foot flat on the mat. Slowly lift torso and rest hands lightly on right thigh. Lean hips forward slightly, keeping right knee behind toes, and feel the stretch in the left hip flexor. Hold here, or for a deeper stretch, raise arms overhead, biceps by ears. Hold for at least 30 seconds, then repeat on opposite side.
Traction involves the use of weights and pulleys to apply constant or intermittent force to gradually “pull” the skeletal structure into better alignment. Some people experience pain relief while in traction, but that relief is usually temporary. Once traction is released the back pain tends to return. There is no evidence that traction provides any longterm benefits for people with low back pain.
^ Jump up to: a b Chou R, Qaseem A, Owens DK, Shekelle P, Clinical Guidelines Committee of the American College of Physicians (1 February 2011). "Diagnostic imaging for low back pain: advice for high-value health care from the American College of Physicians". Annals of Internal Medicine. 154 (3): 181–9. doi:10.7326/0003-4819-154-3-201102010-00008. PMID 21282698.
The medication typically recommended first are NSAIDs (though not aspirin) or skeletal muscle relaxants and these are enough for most people.[13][6] Benefits with NSAIDs; however, is often small.[67] High-quality reviews have found acetaminophen (paracetamol) to be no more effective than placebo at improving pain, quality of life, or function.[68][69] NSAIDs are more effective for acute episodes than acetaminophen; however, they carry a greater risk of side effects including: kidney failure, stomach ulcers and possibly heart problems. Thus, NSAIDs are a second choice to acetaminophen, recommended only when the pain is not handled by the latter. NSAIDs are available in several different classes; there is no evidence to support the use of COX-2 inhibitors over any other class of NSAIDs with respect to benefits.[70][13][71] With respect to safety naproxen may be best.[72] Muscle relaxants may be beneficial.[13]

Strong muscles support and protect your joints. “Strengthening the lower body takes some of the pressure off of the hip and knee joints,” says William Oswald, DPT, a physical therapist and clinical instructor of rehabilitation medicine at NYU Langone Health. This can relieve some of the pain and protect against more damage. “It can also make daily tasks, such as climbing the stairs, easier,” he says.
AAOS does not endorse any treatments, procedures, products, or physicians referenced herein. This information is provided as an educational service and is not intended to serve as medical advice. Anyone seeking specific orthopaedic advice or assistance should consult his or her orthopaedic surgeon, or locate one in your area through the AAOS Find an Orthopaedist program on this website.
MRI and x-ray for low back pain are surprisingly unreliable,1 because things like bulging discs usually aren’t a deal,2 most back pain goes away on its own,3 and trigger points (“muscle knots”) are common and can be alarmingly intense but aren’t dangerous.4 Most patients are much better off when they feel confident about these things. The power of justified, rational confidence is a huge factor in back pain.5 Sadly, many healthcare professionals continue to perpetuate the idea of fragile backs,6 which undermines that valuable confidence.
This Australian study concluded that “prognosis is moderately optimistic for patients with chronic low back pain,” contradicting the common fear that any low back pain that lasts longer than 6-9 weeks will become a long-term chronic problem. This evidence is the first of its kind, a rarity in low back pain research, a field where almost everything has been studied to death. “Many studies provide good evidence for the prognosis of acute low back pain,” the authors explain. “Relatively few provide good evidence for the prognosis of chronic low back pain.”
If the pain is still not managed adequately, short term use of opioids such as morphine may be useful.[73][13] These medications carry a risk of addiction, may have negative interactions with other drugs, and have a greater risk of side effects, including dizziness, nausea, and constipation.[13] The effect of long term use of opioids for lower back pain is unknown.[74] Opioid treatment for chronic low back pain increases the risk for lifetime illicit drug use.[75] Specialist groups advise against general long-term use of opioids for chronic low back pain.[13][76] As of 2016, the CDC has released a guideline for prescribed opioid use in the management of chronic pain.[77] It states that opioid use is not the preferred treatment when managing chronic pain due to the excessive risks involved. If prescribed, a person and their clinician should have a realistic plan to discontinue its use in the event that the risks outweigh the benefit.[77]
Pain along the inside of the hip may be due to tendinitis or strain of the adductor muscles. Adductors (or inner thigh muscles) pull the leg inward as it is moving forward—the faster the movement, the greater the degree of adduction. Since footprints of a runner are almost single file as opposed to the side-by-side footprints of a walker, there is some degree of adduction occurring during running.
Several NIH-funded clinical trials and other studies in patients aim to improve treatment options and prevention strategies for chronic low back pain, as well as add to the evidence base about existing treatments. A multi-year multicenter study called the Spine Patient Outcomes Research Trial (SPORT) compared the most commonly used surgical and nonsurgical treatments for patients with the three most common diagnoses for which spine surgery is performed: intervertebral disc herniation, spinal stenosis, and degenerative spondylisthesis. SPORT represented the largest clinical investigation to date looking at treatment results for these disabling and costly causes of chronic low back pain.
Vertebroplasty and kyphoplasty are minimally invasive treatments to repair compression fractures of the vertebrae caused by osteoporosis. Vertebroplasty uses three-dimensional imaging to assist in guiding a fine needle through the skin into the vertebral body, the largest part of the vertebrae. A glue-like bone cement is then injected into the vertebral body space, which quickly hardens to stabilize and strengthen the bone and provide pain relief. In kyphoplasty, prior to injecting the bone cement, a special balloon is inserted and gently inflated to restore height to the vertebral structure and reduce spinal deformity.

