
So, who cares right? Wrong. Everyone has seen that little old man walking with a cane, hunched over almost to the point of staring at the ground. Do you think he always walked like that? I'd bet you he didn't. Maybe he had an injury that never healed properly, or maybe after spending years and years in a similar position, his body became tighter and tighter until eventually he ended up bent over.
In terms of diagnosing hip pain, typically a patient will expect when they come in to be asked about their symptoms, and it’s very important to find out when did these symptoms start, how long they have been going on, how frequent they are, if they come on in the morning or the evening, do they come on with any certain activity, and if there is something that makes it better or worse. The intensity of the pain is also important. Does it have any associated radiating symptoms? Is it localized in one spot or does it move? After getting a history and finding out what type of pain the patient is having, which also includes whether the pain is dull, aching, sharp, or intense, then it’s important to do a good physical exam. The physical examination involves testing the muscle strength, testing for sensation, doing provocative maneuvers which might help us rule out one type of injury from another.
4. Just swing it. For the front-to-back hip swing stretch, lie on the left side with hips stacked, propped up on the left elbow. Bend the left leg to a 90-degree angle and raise the right leg to hip level with toes pointed. Keep abs tight and swing the right leg all the way in front, then swing it all the way to the back, squeezing the booty along the way. Switch sides.
Behavioral therapy may be useful for chronic pain.[16] There are several types available, including operant conditioning, which uses reinforcement to reduce undesirable behaviors and increase desirable behaviors; cognitive behavioral therapy, which helps people identify and correct negative thinking and behavior; and respondent conditioning, which can modify an individual's physiological response to pain.[17] The benefit however is small.[91] Medical providers may develop an integrated program of behavioral therapies.[17] The evidence is inconclusive as to whether mindfulness-based stress reduction reduces chronic back pain intensity or associated disability, although it suggests that it may be useful in improving the acceptance of existing pain.[92][93]
If you have hip arthritis, work on building up the muscles in your outer thigh for added support. Lie on your pain-free side and lift the leg with arthritis up about six inches, hold for two or three seconds, and lower it again, Humphrey says. Start with one set of 10 repetitions and build up to three sets. Repeat on the other side unless it is too painful. This exercise can aggravate your symptoms if you have hip pain from bursitis.
Poor Sitting Posture: The correct position of your low back should have a slight forward curve called a lordosis. When you sit slouched, this lordosis straightens out-or even worse-reverses itself. This loss of the forward curve in your spine can cause increased pressure on the small shock absorbing discs in your back. This increased pressure can displace your discs and lead to low back pain. Your physical therapist can teach you the proper way to sit to decrease, eliminate, or prevent your back pain.
This standard recommendation reinforces the alarming idea that low back pain that lasts longer than a few weeks is Really Bad News. It’s not. It’s a clue. It’s a reason for concern and alertness. But many cases of low back pain that last for 6 weeks will still go away. Once again, see the 2009 research published in the British Medical Journal, which showed that more than 30% of patients with “new” chronic low back pain will still recover without treatment. BACK TO TEXT
The magnitude of the burden from low back pain has grown worse in recent years. In 1990, a study ranking the most burdensome conditions in the U.S. in terms of mortality or poor health as a result of disease put low back pain in sixth place; in 2010, low back pain jumped to third place, with only ischemic heart disease and chronic obstructive pulmonary disease ranking higher.
Congenital bone conditions: Congenital causes (existing from birth) of low back pain include scoliosis and spina bifida. Scoliosis is a sideways (lateral) curvature of the spine that can be caused when one lower extremity is shorter than the other (functional scoliosis) or because of an abnormal architecture of the spine (structural scoliosis). Children who are significantly affected by structural scoliosis may require treatment with bracing and/or surgery to the spine. Adults infrequently are treated surgically but often benefit by support bracing. Spina bifida is a birth defect in the bony vertebral arch over the spinal canal, often with absence of the spinous process. This birth defect most commonly affects the lowest lumbar vertebra and the top of the sacrum. Occasionally, there are abnormal tufts of hair on the skin of the involved area. Spina bifida can be a minor bony abnormality without symptoms. However, the condition can also be accompanied by serious nervous abnormalities of the lower extremities.
Vertebroplasty and kyphoplasty are minimally invasive treatments to repair compression fractures of the vertebrae caused by osteoporosis. Vertebroplasty uses three-dimensional imaging to assist in guiding a fine needle through the skin into the vertebral body, the largest part of the vertebrae. A glue-like bone cement is then injected into the vertebral body space, which quickly hardens to stabilize and strengthen the bone and provide pain relief. In kyphoplasty, prior to injecting the bone cement, a special balloon is inserted and gently inflated to restore height to the vertebral structure and reduce spinal deformity. 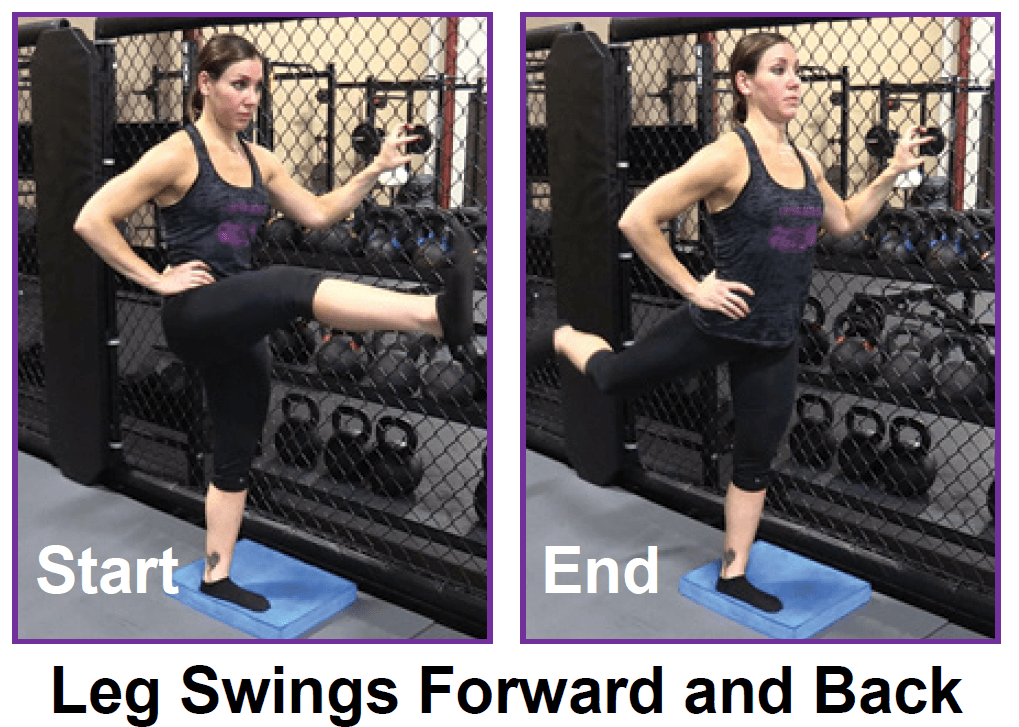
When was the last time you got on your gym's abductor or adductor machine and got in a good workout? It's probably been a while. Both are machines that don't get a lot of use, and they are often the target of coaches' ridicule on those "useless gym moves we should all skip" lists. Perhaps rightly so, especially if you're hopping on those machines hoping for a slimming effect.
While a sharp pain in the hip, groin, pelvis, or thigh is an obvious sign of a hip flexor injury, pain in the lower back and leg are easy to misdiagnose. After all, it’s natural to assume that radiating pain in the leg or lower back originate from these areas. Unfortunately, diagnosing the source of a patient’s pain is not always straightforward. In fact, it’s possible for patients to go years with a misdiagnosed injury.

Low back pain (LBP) is a common disorder involving the muscles, nerves, and bones of the back.[4] Pain can vary from a dull constant ache to a sudden sharp feeling.[4] Low back pain may be classified by duration as acute (pain lasting less than 6 weeks), sub-chronic (6 to 12 weeks), or chronic (more than 12 weeks).[3] The condition may be further classified by the underlying cause as either mechanical, non-mechanical, or referred pain.[5] The symptoms of low back pain usually improve within a few weeks from the time they start, with 40–90% of people completely better by six weeks.[2]
Results after four years of follow-up showed that in general, otherwise healthy people who have surgery for one of these three conditions are likely to fare better than those who receive non-operative care. However, the results also indicated that people who are reluctant to have surgery may also recover with non-operative treatments if their conditions are not progressing and their pain is tolerable, and importantly, delaying or avoiding surgery did not cause additional damage in most cases. Researchers are continuing to track SPORT patient cohorts over a nine-year follow-up period to assess longer term treatment results and cost effectiveness across treatment options. In the interest of improving surgical techniques, NIH also is funding research on factors that contribute to the success or failure of artificial disc replacement surgery, including studies to compare discs on the market for significant differences in their durability rates over time.
Veritas Health publishes original and accessible health related content written by more than 100 physician authors and peer-reviewed by a 16 member Medical Advisory Board. The Veritas Health platform comprising of Spine-health.com, Arthritis-health.com, Sports-health.com, and Pain-health.com, provides comprehensive information on back pain, arthritis, sports injuries, and chronic pain conditions. For more information visit Veritashealth.com.
How to: Position yourself on your hands and knees, in tabletop position. Engage your abs engaged by pulling your belly button in towards your spine (a). Keeping your hips pointed towards the ground and leg bent to a 90-degree angle, raise your left knee out to the side as high as you can (b). Pause at the top, then return to starting position (c). Repeat, then switch legs.
Veritas Health publishes original and accessible health related content written by more than 100 physician authors and peer-reviewed by a 16 member Medical Advisory Board. The Veritas Health platform comprising of Spine-health.com, Arthritis-health.com, Sports-health.com, and Pain-health.com, provides comprehensive information on back pain, arthritis, sports injuries, and chronic pain conditions. For more information visit Veritashealth.com.

In the majority of cases, a hip sprain begins as a microscopic tear that gradually increases in size with repetitive use of the hip. These types of tears are common in sports like cycling, running, swimming, baseball, and golf due to overuse of the hip. If diagnosed early, Grade I and Grade II strains can be effectively treated with rest and other conservative treatments. Grade III strains, however, are one of the most serious hip injuries. This is especially true if the strain is accompanied by a fracture. If your hip cannot bear weight, it is imperative that you contact an orthopaedist for professional treatment.

Degenerative bone and joint conditions: As we age, the water and protein content of the body's cartilage changes. This change results in weaker, thinner, and more fragile cartilage. Because both the discs and the joints that stack the vertebrae (facet joints) are partly composed of cartilage, these areas are subject to wear and tear over time (degenerative changes). Degeneration of the disc is called spondylosis. Spondylosis can be noted on X-rays of the spine as a narrowing of the normal "disc space" between the vertebrae. It is the deterioration of the disc tissue that predisposes the disc to herniation and localized lumbar pain ("lumbago") in older patients. Degenerative arthritis (osteoarthritis) of the facet joints is also a cause of localized lumbar pain that can be detected with plain X-ray testing. These causes of degenerative back pain are usually treated conservatively with intermittent heat, rest, rehabilitative exercises, and medications to relieve pain, muscle spasm, and inflammation.
The medication typically recommended first are NSAIDs (though not aspirin) or skeletal muscle relaxants and these are enough for most people.[13][6] Benefits with NSAIDs; however, is often small.[67] High-quality reviews have found acetaminophen (paracetamol) to be no more effective than placebo at improving pain, quality of life, or function.[68][69] NSAIDs are more effective for acute episodes than acetaminophen; however, they carry a greater risk of side effects including: kidney failure, stomach ulcers and possibly heart problems. Thus, NSAIDs are a second choice to acetaminophen, recommended only when the pain is not handled by the latter. NSAIDs are available in several different classes; there is no evidence to support the use of COX-2 inhibitors over any other class of NSAIDs with respect to benefits.[70][13][71] With respect to safety naproxen may be best.[72] Muscle relaxants may be beneficial.[13] 
Start kneeling on your mat with knees hip-width apart and hips directly over knees. Press your shins and the tops of your feet into the mat. Bring your hands to your low back, fingers pointing down, and rest palms above glutes. Inhale and lift your chest, and then slowly start to lean your torso back. From here, bring your right hand to rest on your right heel and then your left hand to your left heel. (If you can't reach your heels, turn your toes under; it will be easier to reach your heels in this modification.) Press your thighs forward so they are perpendicular to the floor. Keep your head in a relatively neutral position or, if it doesn't strain your neck, drop it back. Hold for 30 seconds. To come out of the pose, bring your hands to your hips and slowly, leading with your chest, lift your torso as you press the thighs down toward the floor.
Stop listening to other people’s horror stories. You know the scenario: You are bent over in obvious pain, waiting to see the doctor, and the person next to you tells you a 10-minute tale of how their Uncle Gordon had low back pain that required injections and surgery. But the pain still didn’t go away. Stop listening to these terrible stories. Most low back pain is short-lived and can be managed quite effectively with exercise and postural correction. Of course, some low back conditions are serious and require surgery, but that is a conversation you should have with your doctor, not the guy in the waiting room.

This stretch gets at the piriformis muscle of the hip flexor. Sit with both legs extended in front of you. Bend the right knee and place the right foot on the floor. Place your right hand behind you and hook your left elbow on the outside of the right knee. As you twist toward the righthand side, keep your spine straight and breathe deeply. Switch sides after about 20 seconds.
Deanna is an ACE® certified personal trainer, Balanced Body® Pilates instructor, and NASM® Fitness Nutrition Specialist. She is passionate about inspiring others to lead a healthier lifestyle through fun workouts and healthy food. When she’s not creating new workouts and recipes for her blog The Live Fit Girls she enjoys running with her two dogs and traveling.

An intervertebral disc has a gelatinous core surrounded by a fibrous ring.[32] When in its normal, uninjured state, most of the disc is not served by either the circulatory or nervous systems – blood and nerves only run to the outside of the disc.[32] Specialized cells that can survive without direct blood supply are in the inside of the disc.[32] Over time, the discs lose flexibility and the ability to absorb physical forces.[25] This decreased ability to handle physical forces increases stresses on other parts of the spine, causing the ligaments of the spine to thicken and bony growths to develop on the vertebrae.[25] As a result, there is less space through which the spinal cord and nerve roots may pass.[25] When a disc degenerates as a result of injury or disease, the makeup of a disc changes: blood vessels and nerves may grow into its interior and/or herniated disc material can push directly on a nerve root.[32] Any of these changes may result in back pain.[32]
Strong muscles support and protect your joints. “Strengthening the lower body takes some of the pressure off of the hip and knee joints,” says William Oswald, DPT, a physical therapist and clinical instructor of rehabilitation medicine at NYU Langone Health. This can relieve some of the pain and protect against more damage. “It can also make daily tasks, such as climbing the stairs, easier,” he says.
If certain activities or overuse are causing hip pain, stop those that aggravate the discomfort and talk to your doctor. Excess weight can put pressure on the hip joint, so losing the pounds can provide relief and help you avoid further problems. Some causes of hip pain, such as fractures or hernias, may need surgical repairs. If your hip pain persists, talk to your doctor about the possible causes and treatments.
In order to validate your account, please either send an email from your .mil email address or send in a snapshot of your military ID to our customer service help desk. Blacking out rank and or post is acceptable. In either case, please include the civilian email address or whichever email address you have registered with Onnit.com somewhere in the message body so we know which account to verify. Please setup an account with Onnit.com prior to submitting your request.
Start in a runner’s lunge, right leg forward with knee over ankle and left knee on ground with top of your foot flat on the mat. Slowly lift torso and rest hands lightly on right thigh. Lean hips forward slightly, keeping right knee behind toes, and feel the stretch in the left hip flexor. Hold here, or for a deeper stretch, raise arms overhead, biceps by ears. Hold for at least 30 seconds, then repeat on opposite side.
^ Dubinsky, R. M.; Miyasaki, J. (2009). "Assessment: Efficacy of transcutaneous electric nerve stimulation in the treatment of pain in neurologic disorders (an evidence-based review): Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology". Neurology. 74 (2): 173–6. doi:10.1212/WNL.0b013e3181c918fc. PMID 20042705.
Initial management with non–medication based treatments is recommended.[6] NSAIDs are recommended if these are not sufficiently effective.[6] Normal activity should be continued as much as the pain allows.[2] Medications are recommended for the duration that they are helpful.[13] A number of other options are available for those who do not improve with usual treatment. Opioids may be useful if simple pain medications are not enough, but they are not generally recommended due to side effects.[4][13] Surgery may be beneficial for those with disc-related chronic pain and disability or spinal stenosis.[14][15] No clear benefit has been found for other cases of non-specific low back pain.[14] Low back pain often affects mood, which may be improved by counseling or antidepressants.[13][16] Additionally, there are many alternative medicine therapies, including the Alexander technique and herbal remedies, but there is not enough evidence to recommend them confidently.[17] The evidence for chiropractic care[18] and spinal manipulation is mixed.[17][19][20][21]
Blood tests are not routinely used to diagnose the cause of back pain; however in some cases they may be ordered to look for indications of inflammation, infection, and/or the presence of arthritis. Potential tests include complete blood count, erythrocyte sedimentation rate, and C-reactive protein. Blood tests may also detect HLA-B27, a genetic marker in the blood that is more common in people with ankylosing spondylitis or reactive arthritis (a form of arthritis that occurs following infection in another part of the body, usually the genitourinary tract).
To ease the pain and lower your odds of an injury, don’t try to do too much at once. “Start with just 10 minutes,” says Arina Garg, MD, a rheumatology fellow at The Center for Excellence for Arthritis and Rheumatology at the Louisiana University Health Sciences Center. “Every few days, increase that time by 5 to 10 minutes.” Your goal is to work up to 30 minutes of aerobic exercise, 5 days a week.
In both younger and older patients, vertebral fractures take weeks to heal with rest and pain relievers. Compression fractures of vertebrae associated with osteoporosis can also be treated with a procedure called vertebroplasty or kyphoplasty, which can help to reduce pain. In this procedure, a balloon is inflated in the compressed vertebra, often returning some of its lost height. Subsequently, a "cement" (methymethacrylate) is injected into the balloon and remains to retain the structure and height of the body of the vertebra. Pain is relieved as the height of the collapsed vertebra is restored.

Spinal fusion eliminates motion between vertebral segments. It is an option when motion is the source of pain. For example, your doctor may recommend spinal fusion if you have spinal instability, a curvature (scoliosis), or severe degeneration of one or more of your disks. The theory is that if the painful spine segments do not move, they should not hurt.
Imaging is indicated when there are red flags, ongoing neurological symptoms that do not resolve, or ongoing or worsening pain.[5] In particular, early use of imaging (either MRI or CT) is recommended for suspected cancer, infection, or cauda equina syndrome.[5] MRI is slightly better than CT for identifying disc disease; the two technologies are equally useful for diagnosing spinal stenosis.[5] Only a few physical diagnostic tests are helpful.[5] The straight leg raise test is almost always positive in those with disc herniation.[5] Lumbar provocative discography may be useful to identify a specific disc causing pain in those with chronic high levels of low back pain.[41] Similarly, therapeutic procedures such as nerve blocks can be used to determine a specific source of pain.[5] Some evidence supports the use of facet joint injections, transforminal epidural injections and sacroilliac injections as diagnostic tests.[5] Most other physical tests, such as evaluating for scoliosis, muscle weakness or wasting, and impaired reflexes, are of little use.[5]
Too much sitting is the enemy of stiff or achy hips, says Lisa Woods, a personal trainer and yoga teacher in Eagle, Colorado. The big problem, though, isn’t just the discomfort in the sides of your thighs. It’s the chain of pain that dysfunctional hips can create, including sciatic nerve pain that can start in your lower back and go down the backs of your legs.

How to: Sit down with your knees bent and feet flat on the floor in front of you (a). Place your right ankle on top of your left thigh and flex your right foot (b). Put your hands behind your body, fingertips facing away from your body and begin to press your hips toward your heels until you feel a stretch through your outer left hip. Keep your back tall and chest open (c). Hold for six to eight breaths, then repeat on the other side. 
When I do a deep knee bend like a sumo squat I get a popping in the outside of my left knee. It feels like a big tendon or ligament is slipping per something. It isn’t painful peer se but I’m afraid if I do it a lot it will be. Is that a relatively common symptom for a guy with tight flexors, it bands, etc? Should I just push through it or have it checked out?

How to do it: Loop a resistance band around your ankles and lie on your right side, supporting your upper body with your right hand and forearm. Extend both legs out, feet flexed. Brace your abs in tight and lift your top leg up to hip height, rotating your leg to turn your toes down to the floor, keeping tension on the band. Lift your leg slightly higher than hip height, pushing against band, with heel rotated up to the ceiling. Return to hip height. Repeat 20 times quickly and then switch sides.
Overall, the outcome for acute low back pain is positive. Pain and disability usually improve a great deal in the first six weeks, with complete recovery reported by 40 to 90%.[2] In those who still have symptoms after six weeks, improvement is generally slower with only small gains up to one year. At one year, pain and disability levels are low to minimal in most people. Distress, previous low back pain, and job satisfaction are predictors of long-term outcome after an episode of acute pain.[2] Certain psychological problems such as depression, or unhappiness due to loss of employment may prolong the episode of low back pain.[13] Following a first episode of back pain, recurrences occur in more than half of people.[23]
Hip labral tear. This is a rip in the ring of cartilage (called the labrum) that follows the outside rim of the socket of your hip joint. Along with cushioning your hip joint, your labrum acts like a rubber seal or gasket to help hold the ball at the top of your thighbone securely within your hip socket. Athletes and people who perform repetitive twisting movements are at higher risk of developing this problem.
MRI and x-ray for low back pain are surprisingly unreliable,1 because things like bulging discs usually aren’t a deal,2 most back pain goes away on its own,3 and trigger points (“muscle knots”) are common and can be alarmingly intense but aren’t dangerous.4 Most patients are much better off when they feel confident about these things. The power of justified, rational confidence is a huge factor in back pain.5 Sadly, many healthcare professionals continue to perpetuate the idea of fragile backs,6 which undermines that valuable confidence.

Chronic back pain is defined as pain that persists for 12 weeks or longer, even after an initial injury or underlying cause of acute low back pain has been treated. About 20 percent of people affected by acute low back pain develop chronic low back pain with persistent symptoms at one year. In some cases, treatment successfully relieves chronic low back pain, but in other cases pain persists despite medical and surgical treatment.
The hip is a basic ball-and-socket joint. The ball is the femoral head—a knob on the top of the thigh bone—and the socket is an indentation in the pelvic bone. There is cartilage lining the joint (called the labrum) and ligaments that attach the pelvic and thigh bones. Numerous muscles attach around the hip, too, moving the joint through the basic motions of flexion (bending), extension (extending the leg behind you), abduction (lifting the leg away from the body), adduction (moving the leg inward), internal rotation, and external rotation.
Women may have acute low back pain from medical conditions affecting the female reproductive system, including endometriosis, ovarian cysts, ovarian cancer, or uterine fibroids.[28] Nearly half of all pregnant women report pain in the lower back or sacral area during pregnancy, due to changes in their posture and center of gravity causing muscle and ligament strain.[29]
Radiculopathy is a condition caused by compression, inflammation and/or injury to a spinal nerve root. Pressure on the nerve root results in pain, numbness, or a tingling sensation that travels or radiates to other areas of the body that are served by that nerve. Radiculopathy may occur when spinal stenosis or a herniated or ruptured disc compresses the nerve root.
The story of actor Andy Whitfield is a disturbing and educational example of a case that met these conditions — for sure the first two, and probably the third as well if we knew the details. Whitfield was the star of the hit TV show Spartacus (which is worthwhile, but rated very, very R17). The first sign of the cancer that killed him in 2011 was steadily worsening back pain. It’s always hard to diagnose a cancer that starts this way, but Whitfield was in the middle of intense physical training to look the part of history’s most famous gladiator. Back pain didn’t seem unusual at first, and some other symptoms may have been obscured. Weight loss could have even seemed like a training victory at first! It was many long months before he was diagnosed — not until the back pain was severe and constant. A scan finally revealed a large tumour pressing against his spine.

Start kneeling on your mat with knees hip-width apart and hips directly over knees. Press your shins and the tops of your feet into the mat. Bring your hands to your low back, fingers pointing down, and rest palms above glutes. Inhale and lift your chest, and then slowly start to lean your torso back. From here, bring your right hand to rest on your right heel and then your left hand to your left heel. (If you can't reach your heels, turn your toes under; it will be easier to reach your heels in this modification.) Press your thighs forward so they are perpendicular to the floor. Keep your head in a relatively neutral position or, if it doesn't strain your neck, drop it back. Hold for 30 seconds. To come out of the pose, bring your hands to your hips and slowly, leading with your chest, lift your torso as you press the thighs down toward the floor.

