
Shingles (herpes zoster) is an acute infection of the nerves that supply sensation to the skin, generally at one or several spinal levels and on one side of the body (right or left). Patients with shingles usually have had chickenpox earlier in life. The herpes virus that causes chickenpox is believed to exist in a dormant state within the spinal nerve roots long after the chickenpox resolves. In people with shingles, this virus reactivates to cause infection along the sensory nerve, leading to nerve pain and usually an outbreak of shingles (tiny blisters on the same side of the body and at the same nerve level). The back pain in patients with shingles of the lumbar area can precede the skin rash by days. Successive crops of tiny blisters can appear for several days and clear with crusty inflammation in one to two weeks. Patients occasionally are left with a more chronic nerve pain (postherpetic neuralgia). Treatment can involve symptomatic relief with lotions, such as calamine, or medications, such as acyclovir (Zovirax), for the infection and pregabalin (Lyrica) or lidocaine (Lidoderm) patches for the pain.

Stop searching for a miracle cure for your back pain. We’ve all seen the advertisements that promise a miracle cure for your low back pain. Hanging by your feet on an inversion table, rubbing healing balms on your back or spending money on fancy computerized traction devices all sound effective but the evidence indicates that many of these miracle cures are not beneficial.
For those with pain localized to the lower back due to disc degeneration, fair evidence supports spinal fusion as equal to intensive physical therapy and slightly better than low-intensity nonsurgical measures.[15] Fusion may be considered for those with low back pain from acquired displaced vertebra that does not improve with conservative treatment,[14] although only a few of those who have spinal fusion experience good results.[15] There are a number of different surgical procedures to achieve fusion, with no clear evidence of one being better than the others.[83] Adding spinal implant devices during fusion increases the risks but provides no added improvement in pain or function.[11]

This Web site provides general educational information on health-related issues and provides access to health-related resources for the convenience of our users. This site and its health-related information and resources are not a substitute for professional medical advice or for the care that patients receive from their physicians or other health care providers.
Pregnancy symptoms can vary from woman to woman, and not all women experience the same symptoms. When women do experience pregnancy symptoms they may include symptoms include missed menstrual period, mood changes, headaches, lower back pain, fatigue, nausea, breast tenderness, and heartburn. Signs and symptoms in late pregnancy include leg swelling and shortness of breath. Options for relief of pregnancy symptoms include exercise, diet, and other lifestyle changes.
Low back pain can cause a wide variety of symptoms and signs depending on the precise cause of the pain as reviewed above. Symptoms that can be associated with low back pain include numbness and/or tingling of the lower extremities, incontinence of urine or stool, inability to walk without worsening pain, lower extremity weakness, atrophy (decreased in size) of the lower extremity muscles, rash, fever, chills, weight loss, abdominal pains, burning on urination, dizziness, joint pain, and fatigue.
Premkumar et al present evidence that the traditional “red flags” for ominous causes of back pain can be quite misleading. The correlation between red flags and ominous diagnoses is poor, and prone to producing false negatives: that is, no red flags even when there is something more serious than unexplained pain going on. In a survey of almost 10,000 patients “the absence of red flag responses did not meaningfully decrease the likelihood of a red flag diagnosis.“ This is not even remotely a surprise to anyone who paid attention in back pain school, but it’s good to have some harder data on it.
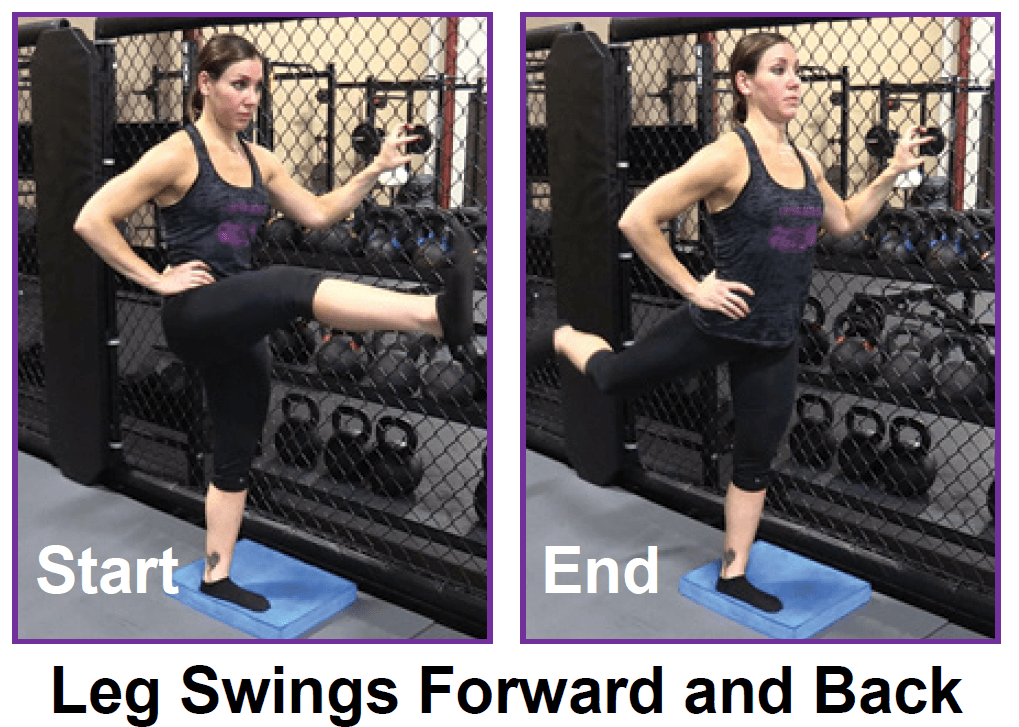
Apply the above concept to your hips. When you sit, your hips are in a "flexed" position. Therefore, the muscles that flex your hips are in a shortened state. You probably spend at least a third of your day sitting down. Think about how much time those hip flexor muscles stay shortened. A lot. Over time, they become tighter and tighter until you look like the old man in the picture. So unless you want to look like that, perform the stretches shown below.

The iliotibial band is a thickening of the fascia lata, the deep fascia of the thigh. Think of it as a thick long ligament like structure that connects the hip to the lower leg along the outside of the thigh. Tightness in the iliotibial band can cause patellofemoral pain, trochanteric bursitis, and friction syndromes at the knee. This is a hip stretch I commonly prescribe to runners and people suffering from knee pain.
How to: Lie on your back with your right knee bent and foot flat on the floor (a). With your left leg fully extended, press into your right foot to shift onto your left hip. This is your starting position (b). Then, squeeze your right glutes to press your left hip open until you feel a stretch, pause, then return to start. That’s one rep (c). Perform six to eight reps, then repeat on the opposite side.

There is controversy and scientific uncertainty about trigger points. It’s undeniable that mammals suffer from sensitive spots in our soft tissues … but their nature remains unclear, and the “tiny cramp” theory could be wrong. The tiny cramp theory is formally known as the “expanded integrated hypothesis,” and it has been prominently criticized by Quintner et al (and not many others). However, it’s the mostly widely accepted explanation for now. BACK TO TEXT
Stop focusing on a specific diagnosis. Up to 85% of low back pain can be classified as "non-specific." This means that the origin of your pain cannot be localized to one specific structure or problem. While common diagnostic tests for low back pain can show the bones, discs, and joints with great detail, no test can tell the exact cause of your pain with 100% accuracy. 
Behavioral therapy may be useful for chronic pain.[16] There are several types available, including operant conditioning, which uses reinforcement to reduce undesirable behaviors and increase desirable behaviors; cognitive behavioral therapy, which helps people identify and correct negative thinking and behavior; and respondent conditioning, which can modify an individual's physiological response to pain.[17] The benefit however is small.[91] Medical providers may develop an integrated program of behavioral therapies.[17] The evidence is inconclusive as to whether mindfulness-based stress reduction reduces chronic back pain intensity or associated disability, although it suggests that it may be useful in improving the acceptance of existing pain.[92][93]
There is a significant overlap of nerve supply to many of the discs, muscles, ligaments, and other spinal structures, and it can be difficult for the brain to accurately sense which is the cause of the pain. For example, a degenerated or torn lumbar disc can feel the same as a pulled muscle – both creating inflammation and painful muscle spasm in the same area. Muscles and ligaments heal rapidly, while a torn disc may or may not. The time course of pain helps determine the cause.

Intradiscal electrothermal therapy (IDET) is a treatment for discs that are cracked or bulging as a result of degenerative disc disease. The procedure involves inserting a catheter through a small incision at the site of the disc in the back. A special wire is passed through the catheter and an electrical current is applied to heat the disc, which helps strengthen the collagen fibers of the disc wall, reducing the bulging and the related irritation of the spinal nerve. IDET is of questionable benefit.
Tight hip flexors can result in lower back pain, hip pain and injury. A lot of strain is put on those muscles during activities that involve sprinting and kicking. For example, runners are more prone to hip flexor injuries because of the small, repetitive movement during running. But even if you’re not an athlete, hip flexor injuries can occur during everyday activities (for instance, slipping and falling or running to catch a bus). When those tight muscles are suddenly stretched beyond what they are accustomed to, you might also experience pain in the upper groin region, typically where the hip meets the pelvis.
Lumbar radiculopathy: Lumbar radiculopathy is nerve irritation that is caused by damage to the discs between the vertebrae. Damage to the disc occurs because of degeneration ("wear and tear") of the outer ring of the disc, traumatic injury, or both. As a result, the central softer portion of the disc can rupture (herniate) through the outer ring of the disc and abut the spinal cord or its nerves as they exit the bony spinal column. This rupture is what causes the commonly recognized "sciatica" pain of a herniated disc that shoots from the low back and buttock down the leg. Sciatica can be preceded by a history of localized low-back aching or it can follow a "popping" sensation and be accompanied by numbness and tingling. The pain commonly increases with movements at the waist and can increase with coughing or sneezing. In more severe instances, sciatica can be accompanied by incontinence of the bladder and/or bowels. The sciatica of lumbar radiculopathy typically affects only one side of the body, such as the left side or right side, and not both. Lumbar radiculopathy is suspected based on the above symptoms. Increased radiating pain when the lower extremity is lifted supports the diagnosis. Nerve testing (EMG/electromyogramspina bifida

Congenital bone conditions: Congenital causes (existing from birth) of low back pain include scoliosis and spina bifida. Scoliosis is a sideways (lateral) curvature of the spine that can be caused when one lower extremity is shorter than the other (functional scoliosis) or because of an abnormal architecture of the spine (structural scoliosis). Children who are significantly affected by structural scoliosis may require treatment with bracing and/or surgery to the spine. Adults infrequently are treated surgically but often benefit by support bracing. Spina bifida is a birth defect in the bony vertebral arch over the spinal canal, often with absence of the spinous process. This birth defect most commonly affects the lowest lumbar vertebra and the top of the sacrum. Occasionally, there are abnormal tufts of hair on the skin of the involved area. Spina bifida can be a minor bony abnormality without symptoms. However, the condition can also be accompanied by serious nervous abnormalities of the lower extremities.

Vertebroplasty and kyphoplasty are minimally invasive treatments to repair compression fractures of the vertebrae caused by osteoporosis. Vertebroplasty uses three-dimensional imaging to assist in guiding a fine needle through the skin into the vertebral body, the largest part of the vertebrae. A glue-like bone cement is then injected into the vertebral body space, which quickly hardens to stabilize and strengthen the bone and provide pain relief. In kyphoplasty, prior to injecting the bone cement, a special balloon is inserted and gently inflated to restore height to the vertebral structure and reduce spinal deformity.
Magnetic resonance imaging (MRI) uses a magnetic force instead of radiation to create a computer-generated image. Unlike x-ray, which shows only bony structures, MRI scans also produce images of soft tissues such as muscles, ligaments, tendons, and blood vessels. An MRI may be ordered if a problem such as infection, tumor, inflammation, disc herniation or rupture, or pressure on a nerve is suspected. MRI is a noninvasive way to identify a condition requiring prompt surgical treatment. However, in most instances, unless there are “red flags” in the history or physical exam, an MRI scan is not necessary during the early phases of low back pain.

With the stakes so high, doesn’t it make sense to do all you can to strengthen and protect your hips? Even if you have arthritis in a hip — the reason for 8 in 10 replacements — you may be able to manage pain with exercise. In a 2017 pilot study published in the Journal of Osteoporosis, women 65 and older who exercised three times a week in a supervised 12-week program reduced arthritic hip pain by over 30 percent, with similar gains in strength, and joint range of motion. The four exercises here will fortify the muscles that surround and support your hips, says trainer Robert Linkul, owner of Be Stronger Fitness in Sacramento, Calif. He advises doing these simple moves, two to three sets of five to 10 reps each, three times a week. Compare how you feel after three weeks.
Pain along the inside of the hip may be due to tendinitis or strain of the adductor muscles. Adductors (or inner thigh muscles) pull the leg inward as it is moving forward—the faster the movement, the greater the degree of adduction. Since footprints of a runner are almost single file as opposed to the side-by-side footprints of a walker, there is some degree of adduction occurring during running.
Spinal fusion is used to strengthen the spine and prevent painful movements in people with degenerative disc disease or spondylolisthesis (following laminectomy). The spinal disc between two or more vertebrae is removed and the adjacent vertebrae are “fused” by bone grafts and/or metal devices secured by screws. The fusion can be performed through the abdomen, a procedure known as an anterior lumbar interbody fusion, or through the back, called posterior fusion. Spinal fusion may result in some loss of flexibility in the spine and requires a long recovery period to allow the bone grafts to grow and fuse the vertebrae together. Spinal fusion has been associated with an acceleration of disc degeneration at adjacent levels of the spine.
This Web site provides general educational information on health-related issues and provides access to health-related resources for the convenience of our users. This site and its health-related information and resources are not a substitute for professional medical advice or for the care that patients receive from their physicians or other health care providers.
Stop focusing on a specific diagnosis. Up to 85% of low back pain can be classified as "non-specific." This means that the origin of your pain cannot be localized to one specific structure or problem. While common diagnostic tests for low back pain can show the bones, discs, and joints with great detail, no test can tell the exact cause of your pain with 100% accuracy.

The hip joint is designed to withstand a fair amount of wear and tear, but it’s not indestructible. For example, when you walk, a cushion of cartilage helps prevent friction as the hip bone moves in its socket. With age and use, this cartilage can wear down or become damaged, or the hip bone itself can be fractured during a fall. In fact, more than 300,000 adults over 65 are hospitalized for hip fractures each year, according to the Agency for Healthcare Research and Quality.

These are really great tips. Just to imform my friends here, my cousin also gave me this link about some other techniches you can use. You have to know exactly what is going on in your body you know. the product is called Panifix, or "Unlock your hip flexor" which Gives You A Practical, Easy-to-follow Program You Can Use To Instantly Release Your Hip Flexors For More Strength, Better Health And All Day Energy. Proven Swipes And Creatives Here:https://tinyurl.com/yd6nbzfh
When I do a deep knee bend like a sumo squat I get a popping in the outside of my left knee. It feels like a big tendon or ligament is slipping per something. It isn’t painful peer se but I’m afraid if I do it a lot it will be. Is that a relatively common symptom for a guy with tight flexors, it bands, etc? Should I just push through it or have it checked out?

