
How to do it: Loop a resistance band around your ankles and lie on your right side with your right arm extended on the floor, left hand in front of your body for support. Brace your abs in tight, bring your bottom leg slightly in front of your top leg (let the inside of your top foot rest on the ground), and lift your leg up to the ceiling, keeping your hips stacked. Maintain tension on the band at all times and pulse your bottom leg up and down quickly 20 times. Repeat on the other side.
Imaging is indicated when there are red flags, ongoing neurological symptoms that do not resolve, or ongoing or worsening pain.[5] In particular, early use of imaging (either MRI or CT) is recommended for suspected cancer, infection, or cauda equina syndrome.[5] MRI is slightly better than CT for identifying disc disease; the two technologies are equally useful for diagnosing spinal stenosis.[5] Only a few physical diagnostic tests are helpful.[5] The straight leg raise test is almost always positive in those with disc herniation.[5] Lumbar provocative discography may be useful to identify a specific disc causing pain in those with chronic high levels of low back pain.[41] Similarly, therapeutic procedures such as nerve blocks can be used to determine a specific source of pain.[5] Some evidence supports the use of facet joint injections, transforminal epidural injections and sacroilliac injections as diagnostic tests.[5] Most other physical tests, such as evaluating for scoliosis, muscle weakness or wasting, and impaired reflexes, are of little use.[5]

There are many causes of hip joint pain. Some hip pain is temporary, while other hip pain can be long-standing or chronic. Causes of hip pain include arthritis, inflammatory and noninflammatory arthritis, fracture, sprain, infectious arthritis (septic arthritis), avascular necrosis, Gaucher's disease, sciatica, muscle strain, iliotibial band syndrome (IT band syndrome), and hematoma.
Compressive pain is a result of pressure or irritation on the spinal cord, nerves that leave the spine. For example, if an intervertebral disc herniates (usually called a ruptured disc) and pushes into the spinal canal, it can cause problems with the nerve. Usually this pressure or irritation causes pain, numbness, and muscle weakness where the nerve travels.

I am a science writer, former massage therapist, and I was the assistant editor at ScienceBasedMedicine.org for several years. I have had my share of injuries and pain challenges as a runner and ultimate player. My wife and I live in downtown Vancouver, Canada. See my full bio and qualifications, or my blog, Writerly. You might run into me on Facebook or Twitter.

Long periods of inactivity in bed are no longer recommended, as this treatment may actually slow recovery. Spinal manipulation for periods of up to one month has been found to be helpful in some patients who do not have signs of nerve irritation. Future injury is avoided by using back-protection techniques during activities and support devices as needed at home or work.
For those with pain localized to the lower back due to disc degeneration, fair evidence supports spinal fusion as equal to intensive physical therapy and slightly better than low-intensity nonsurgical measures.[15] Fusion may be considered for those with low back pain from acquired displaced vertebra that does not improve with conservative treatment,[14] although only a few of those who have spinal fusion experience good results.[15] There are a number of different surgical procedures to achieve fusion, with no clear evidence of one being better than the others.[83] Adding spinal implant devices during fusion increases the risks but provides no added improvement in pain or function.[11]

Your hip labrum is a band of cartilage-like tissue that courses around the outer rim of your hip socket. This labrum helps to support the joint and deepen the socket. Sometimes overuse or an injury to your hip can cause a tear in your labrum. A hip labrum tear may result in a condition called femoroacetabular impingement (FAI). When this happens, hip pain may result, and exercises to stretch and stabilize your hip may be performed.
Electrodiagnostics are procedures that, in the setting of low back pain, are primarily used to confirm whether a person has lumbar radiculopathy. The procedures include electromyography (EMG), nerve conduction studies (NCS), and evoked potential (EP) studies. EMG assesses the electrical activity in a muscle and can detect if muscle weakness results from a problem with the nerves that control the muscles. Very fine needles are inserted in muscles to measure electrical activity transmitted from the brain or spinal cord to a particular area of the body. NCSs are often performed along with EMG to exclude conditions that can mimic radiculopathy. In NCSs, two sets of electrodes are placed on the skin over the muscles. The first set provides a mild shock to stimulate the nerve that runs to a particular muscle. The second set records the nerve’s electrical signals, and from this information nerve damage that slows conduction of the nerve signal can be detected. EP tests also involve two sets of electrodes—one set to stimulate a sensory nerve, and the other placed on the scalp to record the speed of nerve signal transmissions to the brain. 
Bridge: Still lying on your back with your feet flat on floor, lift your hips and torso off the floor into a bridge. Then interlace your hands underneath your hips and press your shoulders and upper arms into the floor, lifting your hips higher. Hold for 10 seconds. Lower yourself slowly back down, rolling down from the top of your spine to your tailbone. Repeat three times.
Increasing general physical activity has been recommended, but no clear relationship to pain or disability has been found when used for the treatment of an acute episode of pain.[48][54] For acute pain, low- to moderate-quality evidence supports walking.[55] Treatment according to McKenzie method is somewhat effective for recurrent acute low back pain, but its benefit in the short term does not appear significant.[1] There is tentative evidence to support the use of heat therapy for acute and sub-chronic low back pain[56] but little evidence for the use of either heat or cold therapy in chronic pain.[57] Weak evidence suggests that back belts might decrease the number of missed workdays, but there is nothing to suggest that they will help with the pain.[50] Ultrasound and shock wave therapies do not appear effective and therefore are not recommended.[58][59] Lumbar traction lacks effectiveness as an intervention for radicular low back pain.[60]
Without changing the position of your knees, bend at your hips and lower your torso until it’s almost parallel to the floor (or as far as you can comfortably go without rounding your back). Pause, then lift your torso back to the starting position. Be sure to squeeze your glutes and push your hips forward to lift your torso back to the starting position. This ensures you’re engaging your hip muscles instead of relying on your lower back. Do 10 reps total.
How to: Lie on your back with your right knee bent and foot flat on the floor (a). With your left leg fully extended, press into your right foot to shift onto your left hip. This is your starting position (b). Then, squeeze your right glutes to press your left hip open until you feel a stretch, pause, then return to start. That’s one rep (c). Perform six to eight reps, then repeat on the opposite side.

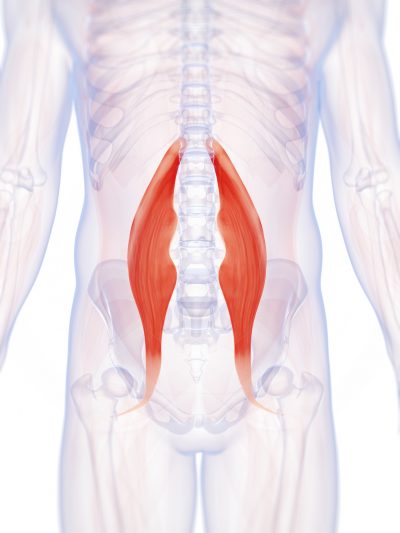
Really a great content. Let me tell you first about hip flexor it is the engine through which our body moves. They control balance, our ability to sit, stand, twist, reach, bend, walk and step. One of my patient also suffering from same problem but due to lack of money he was unable to afford a treatment. So i recommend him a program to unlock hip flexor. If anyone wants they can check it out here ;- https://tinyurl.com/y8yaqs2s Report
This stretch gets at the piriformis muscle of the hip flexor. Sit with both legs extended in front of you. Bend the right knee and place the right foot on the floor. Place your right hand behind you and hook your left elbow on the outside of the right knee. As you twist toward the righthand side, keep your spine straight and breathe deeply. Switch sides after about 20 seconds.
Men and women are equally affected by low back pain, which can range in intensity from a dull, constant ache to a sudden, sharp sensation that leaves the person incapacitated. Pain can begin abruptly as a result of an accident or by lifting something heavy, or it can develop over time due to age-related changes of the spine. Sedentary lifestyles also can set the stage for low back pain, especially when a weekday routine of getting too little exercise is punctuated by strenuous weekend workout.
Two types of strength-training moves that may benefit the lower back are flexion and extension exercises. In flexion exercises, you bend forward to stretch the muscles of the back and hips. In extension exercises, you bend backward to develop the muscles that support the spine. One example is doing leg lifts while lying on your stomach. Depending on the cause of your back pain, there are some exercises you should not do. If you have back pain, make sure to talk to your doctor about what exercises are safe for you.
Bridge: Still lying on your back with your feet flat on floor, lift your hips and torso off the floor into a bridge. Then interlace your hands underneath your hips and press your shoulders and upper arms into the floor, lifting your hips higher. Hold for 10 seconds. Lower yourself slowly back down, rolling down from the top of your spine to your tailbone. Repeat three times.
Exercise appears to be useful for preventing low back pain.[47] Exercise is also probably effective in preventing recurrences in those with pain that has lasted more than six weeks.[1][48] Medium-firm mattresses are more beneficial for chronic pain than firm mattresses.[49] There is little to no evidence that back belts are any more helpful in preventing low back pain than education about proper lifting techniques.[47][50] Shoe insoles do not help prevent low back pain.[47][51]

The condition is cauda equina syndrome. It involves “acute loss of function of the neurologic elements (nerve roots) of the spinal canal below the termination (conus) of the spinal cord,” where the nerves spread out like a horse (equina) tail. Again, this condition causes symptoms in the “saddle” of the body: butt, groin, inner thighs. BACK TO TEXT
Disc degeneration remains a key cause of chronic low back pain and the pain often persists despite surgery. NIH-funded basic science and preclinical studies are investigating molecular-level mechanisms that cause discs in the spine to degenerate, as well as protective mechanisms involved in disc remodeling that may diminish with advancing age. Such studies may help identify future therapeutic strategies to block degenerative mechanisms or promote remodeling processes. NIH also is funding early research on stem cell approaches to promote disc regeneration and rejuvenate cells of the nucleus pulposus, the jelly-like substance in the center of intervertebral discs that loses water content as people age.
In terms of diagnosing hip pain, typically a patient will expect when they come in to be asked about their symptoms, and it’s very important to find out when did these symptoms start, how long they have been going on, how frequent they are, if they come on in the morning or the evening, do they come on with any certain activity, and if there is something that makes it better or worse. The intensity of the pain is also important. Does it have any associated radiating symptoms? Is it localized in one spot or does it move? After getting a history and finding out what type of pain the patient is having, which also includes whether the pain is dull, aching, sharp, or intense, then it’s important to do a good physical exam. The physical examination involves testing the muscle strength, testing for sensation, doing provocative maneuvers which might help us rule out one type of injury from another.

Start kneeling on your mat with knees hip-width apart and hips directly over knees. Press your shins and the tops of your feet into the mat. Bring your hands to your low back, fingers pointing down, and rest palms above glutes. Inhale and lift your chest, and then slowly start to lean your torso back. From here, bring your right hand to rest on your right heel and then your left hand to your left heel. (If you can't reach your heels, turn your toes under; it will be easier to reach your heels in this modification.) Press your thighs forward so they are perpendicular to the floor. Keep your head in a relatively neutral position or, if it doesn't strain your neck, drop it back. Hold for 30 seconds. To come out of the pose, bring your hands to your hips and slowly, leading with your chest, lift your torso as you press the thighs down toward the floor.

